US China Neuro Exchange 美中神经交流
Progress Note 2
KEY WORDS
NOTE
40 y o man who was found down by his family at home. Brought to the emergency room by the paramedics with a Glascow Coma Score
The patient has chronic renal failure for more than 20 years secondary to diabetes mellitus and receives dialysis weekly.
Currently his vital signs are HR 65, Sbp 97/54. On a ventilator on synchronous intermittent mechanical ventilation at a rate of 14. (The patient is not breathing over the ventilator rate).
He has a hard collar (his C-spine is not yet cleared because he cannot say whether or not he has neck pain and cannot cooperate with flexion extension films).
His lungs are clear to auscultation. Heart is regular with no murmurs. Abdomen is soft and non-tender. He has a nasogastric tube which is clamped shut. He has bowel sounds. The skin of his back, hips, and buttock is intact. There is no lower extremity swelling. Neurologically he is comatose with a Glascow Coma Score of 3. He has only a weak cough and gag. Right pupil size and reactivity impossible to assess due to cataract. Left pupil is 6 mm and non-reactive.
Fluids electrolytes nutrition: IV fluid normal saline with 20 mEq/liter at 10 cc per hour (because he is on dialysis). He is also receiving 3% normal saline at 100 cc/hr. He has a foley catheter in place but his urine output has been 0 cc/hr for several hours and was only 5 cc overnight. This morning his sodium is 137 mEq per liter, his potassium is 3.7 mEq/liter. BUN is 73, creatinine 13.3. Dialysis was attempted this morning but had to be aborted due to hypotension. Plan is for a Renal consultation to help coordinate future dialysis treatements.
Respiratory: His most recent arterial blood gas shows a pH of 7.54, bicarbonate of 23 mmole/liter, and a pCO2 of 27 mmHg. His pO2 is 116 mmHg on 40%.
Cardiovascular: No current issues or concerns.
Gastrointestinal: No nasogastric drainage at this time.
Urinary: No urine output at this time. Foley in place, monitoring urine output.
Hematologic: This morning his hematocrit is 27.8%.
Infection: No fevers now or in past 24 hours. White blood cell count is 10.2 thousand per cubic mm.
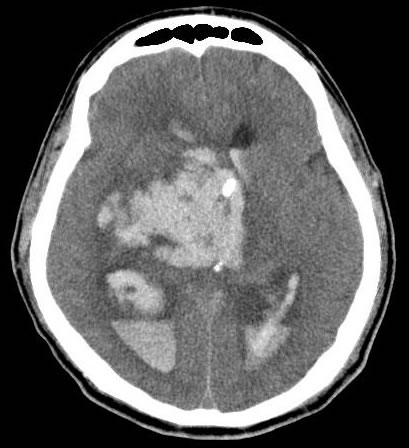
Neurologic: patient has an external ventricular drain. Intracranial pressure is currently 8.
Assessment:
1. devastating massive intracerebral hemorrhage etiology unknown but most likely due to long-standing hypertensive angiopathy. No surgical evacuation contemplated because blood is in brain tissue and ventricles throughout the brain. If patient's intracranial pressure rises and cannot be controlled with medical management, he may be a candidate for decompressive craniectomy.
2. Very poor prognosis for neurologic recovery given GCS of 3 and unreactive pupil.
2. renal failure is major medical concern
Plan:
1. normalize the pCO2 and pH by letting the CO2 increase by decreasing ventilator rate.
2. start enteral feedings as soon as patient can tolerate as evidenced by low nasogastric residuals.
3. follow recommendations of renal consult
4. discuss prognosis with family.
男子40哟谁发现了他在国内的家人失望。带到了格拉斯哥昏迷评分急诊室的医护人员
病人有慢性超过20年继发于糖尿病和肾功能衰竭透析每周接收。
目前他的生命体征65小时,收缩压五十四分之九十七。一项关于同步间歇机械通风率在14呼吸器。 (病人不超过呼吸器呼吸率)。
他有一个硬领(他的C -脊柱尚未结清,因为他不能说他是否有颈部疼痛,不能屈伸合作扩展电影)。
他的肺部听诊无杂音。心正则,无杂音。腹部是软的,非标件。他有一个鼻胃管这是钳制关闭。他有肠鸣音。他的背部,臀部和臀部皮肤完好。没有下肢肿胀。神经学,就是和格拉斯哥昏迷昏迷3分。他只是一个弱咳嗽和作呕。右瞳孔大小和反应性无法评估,由于白内障。左瞳孔为6毫米和非反应性。
电解质营养液:静脉输液生理盐水20毫克当量/每小时10毫升(因为他在透析)升。他也获得100毫升/小时3%生理盐水。他在地方Foley导尿管,但他的尿量已被0毫升/小时几个小时,只有5毫升过夜。今天早上他钠是每升137毫克当量,钾为3.7毫克当量他/升。尿素氮为73,肌酐13.3。今天早上试图透析而不得不中止因低血压。计划是一个咨询,帮助协调肾透析treatements未来。
呼吸系统:他最近的动脉血气显示了7.54 pH值,碳酸氢钠23 mmole /升,和27毫米汞柱的pCO2。他的氧分压为116毫米汞柱40%。
心血管:没有当前的问题或疑虑。
胃肠道:目前没有鼻胃管引流。
泌尿:没有在这个时候尿量。弗利到位,监测尿量。
血液学:今天上午他的血细胞比容为27.8%。
感染:现在没有发烧或过去24个小时。白细胞计数每立方毫米为10.2万。
神经系统:患者有一个外部心室流失。目前8颅内压。
评估:
1。大规模毁灭性的病因不明,但脑出血的最可能是由于长期高血压血管病变。无手术疏散考虑,因为脑组织的血液和整个脑室的。如果病人的颅内压力上升,并且不能与医疗管理控制,他可能是去骨瓣减压候选人。
2。对于神经功能恢复由于反应活性GCS评分为3和预后差的学生。
2。肾功能衰竭是主要的医疗问题
计划:
1。通过让正常化通过降低呼吸速率增加二氧化碳pCO2和pH值。
2。开始肠内喂养只要病人能容忍低鼻胃管残差证明。
3。按照建议征询肾
4。与家人讨论预后。